

Introduction: Lenalidomide (LEN), a standard of care for newly diagnosed multiple myeloma, is routinely administered until disease progression. However, patients with disease that has relapsed after or become refractory to LEN have been poorly represented in recent trials investigating triplet regimens after ≤ 3 prior treatment (Tx) lines. Consequently, patients who have exhausted the benefits of LEN in early relapse are a clinically relevant population in need of proven Tx options. The trial that led to approval of pomalidomide (POM) + dexamethasone (DEX) + daratumumab (DARA) evaluated patients with heavily pretreated (median of 4 prior lines of therapy) relapsed refractory multiple myeloma (RRMM; Chari et al. Blood 2017). The phase 2 MM-014 trial (NCT01946477), which is composed of 3 cohorts, was specifically designed to investigate the outcomes of sequencing POM-based therapy immediately after first- or second-line LEN-based Tx failure in patients with RRMM. In an earlier report from cohort B of MM-014, POM + DEX + DARA demonstrated promising efficacy and safety results: the overall response rate (ORR) was 77.7%, and the 1-year progression-free survival (PFS) rate was 75.1% at a median follow-up of 17.2 months (Siegel et al. Leukemia 2020). Updated efficacy and safety results from cohort B are reported here.
Methods: Patients with RRMM treated with 1-2 prior Tx lines, LEN-based Tx as their most recent regimen, and progressive disease during/after their last line of Tx received POM + DEX + DARA. POM 4 mg/day was given orally on days 1-21; DEX 40 mg/day (20 mg/day in patients aged > 75 years) was given orally on days 1, 8, 15, and 22; and DARA 16 mg/kg was given intravenously on days 1, 8, 15, and 22 of cycles 1 and 2, days 1 and 15 for cycles 3-6, and day 1 for cycles 7+. ORR was the primary endpoint; secondary endpoints included PFS and safety.
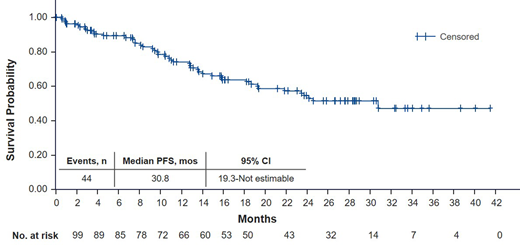
Results: In the intention-to-treat (ITT) population of 112 patients, the median age was 66.5 years, all patients had prior LEN, and 77.7% had prior bortezomib. Overall, 84 patients (75%) had LEN-refractory MM and 28 (25%) had MM that relapsed after prior LEN Tx; most patients (70 [62.5%]) received 1 vs 2 (42 [37.5%]) prior Tx lines. As of March 24, 2020, 31 patients (27.7%) were still on treatment; median follow-up was 28.4 months. The most common reasons for discontinuation in 81 patients (72.3%) were progressive disease (46 patients [56.8%]), withdrawal by patient (19 patients [23.5%]), and adverse events (AEs; 7 patients [8.6%]). The efficacy-evaluable (EE) population comprised 109 patients who received ≥ 1 dose of study Tx and had ≥ 1 post-baseline assessment and was used for supportive efficacy analyses. ORR was 77.7% (≥ very good partial response [VGPR], 52.7%) and 79.8% (≥ VGPR, 54.1%) in the ITT and EE populations, respectively. ORR was similar in patients with LEN-relapsed and LEN-refractory disease (82.1% and 76.2%, respectively). The median PFS was reached: 30.8 months in both the ITT and EE populations (Figure). Overall, 97.3% of patients had ≥ 1 grade 3/4 AE, with neutropenia (64.3%; febrile 9.8%) being the most common grade 3/4 hematologic Tx-emergent AE, followed by anemia (17.9%) and thrombocytopenia (14.3%). Grade 3/4 infections were noted in 36.6% of patients, including 16.1% with grade 3/4 pneumonia.
Conclusions: POM + DEX + DARA administered in early-line Tx immediately after LEN failure continues to show a high response rate and a consistent safety profile, demonstrating the benefit of maintaining continuous immunomodulation with POM following LEN. These updated results continue to demonstrate the efficacy and safety of POM-based therapy as early as second line in patients with RRMM, even immediately after LEN failure, indicating that switching from the immunomodulatory agent class is not necessary. Furthermore, these findings support the use of POM + DEX as the foundation of novel combinations in MM.
Siegel:Karyopharma: Consultancy, Honoraria; Takeda: Consultancy, Honoraria, Speakers Bureau; BMS: Consultancy, Honoraria, Speakers Bureau; Janssen: Consultancy, Honoraria, Speakers Bureau; Merck: Consultancy, Honoraria, Speakers Bureau; Amgen: Consultancy, Honoraria, Speakers Bureau; Celulatiry: Consultancy. Schiller:Forma: Research Funding; Bristol-Myers Squibb: Current equity holder in publicly-traded company, Research Funding; Deciphera: Research Funding; DeltaFly: Research Funding; Regimmune: Research Funding; Samus: Research Funding; Sangamo: Research Funding; Tolero: Research Funding; Trovagene: Research Funding; Kaiser Permanente: Consultancy; Johnson & Johnson: Current equity holder in publicly-traded company; FujiFilm: Research Funding; Mateon: Research Funding; Kite Pharma: Research Funding; Karyopharm: Research Funding; Celator: Research Funding; Constellation: Research Funding; Cyclacel: Research Funding; Jazz Pharmaceuticals: Research Funding; Agios: Consultancy, Research Funding, Speakers Bureau; Incyte: Consultancy, Research Funding, Speakers Bureau; AstraZeneca: Consultancy; Amgen: Consultancy, Current equity holder in publicly-traded company, Research Funding, Speakers Bureau; Novartis: Consultancy, Research Funding; Ono Pharma: Consultancy; Celgene: Research Funding, Speakers Bureau; Sanofi: Speakers Bureau; Gilead: Speakers Bureau; Astellas Pharma: Honoraria, Research Funding; Ariad: Research Funding; Actinium: Research Funding; Abbvie: Research Funding; Stemline: Speakers Bureau; Pfizer: Current equity holder in publicly-traded company, Research Funding; MedImmune: Research Funding; Onconova: Research Funding; Daiichi Sankyo: Research Funding; Geron: Research Funding; Genentech-Roche: Research Funding; Gamida: Research Funding. Sebag:Celgene: Honoraria; Takeda: Honoraria; Amgen: Honoraria; Janssen: Honoraria, Research Funding. Berdeja:CRISPR Therapeutics: Consultancy, Research Funding; Cellularity: Research Funding; Celgene: Consultancy, Research Funding; Servier: Consultancy; Teva: Research Funding; Prothena: Consultancy; BMS: Consultancy, Research Funding; Takeda: Consultancy, Research Funding; Bioclinica: Consultancy; Bluebird: Research Funding; Vivolux: Research Funding; Abbvie: Research Funding; Amgen: Consultancy, Research Funding; Acetylon: Research Funding; Poseida: Research Funding; CURIS: Research Funding; EMD Sorono: Research Funding; Genentech, Inc.: Research Funding; Glenmark: Research Funding; Janssen: Consultancy, Research Funding; Karyopharm: Consultancy; Kesios: Research Funding; Kite Pharma: Consultancy; Legend: Consultancy; Lilly: Research Funding; Novartis: Research Funding; Constellation: Research Funding. Ganguly:KITE Pharma: Speakers Bureau; Settle Genetics: Speakers Bureau; Kadmon: Other: Ad Board. Matous:Bristol-Myers Squibb Company: Consultancy, Honoraria, Speakers Bureau. Song:Celgene: Research Funding; Celgene, Janssen, Amgen, Takeda: Honoraria. Bar:Bristol-Myers Squibb Company: Consultancy. Anz:AbbVie: Other: Investigator in AbbVie-sponsored clinical trials. Fonseca:Bristol-Myers Squibb Company: Speakers Bureau. Reece:Janssen, Bristol-Myers Squibb: Membership on an entity's Board of Directors or advisory committees; Merck: Honoraria, Research Funding; Otsuka: Research Funding; Janssen, Bristol-Myers Squibb, Amgen, Takeda: Consultancy, Honoraria. Lee:Bristol-Myers Squibb Company: Current Employment, Current equity holder in publicly-traded company. Agarwal:Bristol-Myers Squibb Company: Current Employment, Current equity holder in publicly-traded company. Bahlis:BMS/Celgene and Janssen: Consultancy, Honoraria, Other: Travel, Accomodations, Research Funding; Takeda: Consultancy, Honoraria; Amgen: Consultancy, Honoraria; GSK: Consultancy, Honoraria; Genentech: Consultancy, Honoraria; AbbVie: Consultancy, Honoraria; Karyopharm Therapeutics: Consultancy, Honoraria; Sanofi: Consultancy, Honoraria.

